Bad posture; common examples of poor posture.

Contents
This article has been written to highlight some of the more common examples of bad posture that I see almost every day. It gives a brief description and example of each type and lists the effected muscles (when applicable).
I am planning to write individual articles on some of these problems and will provide links from this page when they are written. In this article, I will concentrate on static standing alignment and leave sitting and sleeping posture for another time.
Throughout this article, I will be using some anatomical terms and proper muscle names. The human body is complicated and its pretty difficult to explain posture without using the correct terminology. I’ve tried to keep it relatively jargon free. There may however be times where you may have to Google a term or muscle name to see what I am talking about. Learning more about a problem and fixing it, often takes a bit of homework.
Bad posture
Firstly, I think it’s important to point out, that almost nobody has perfect posture. Bad posture in all its forms is incredibly common. I have yet to assess anyone without finding at least a couple of things wrong. Most of us have something going on somewhere.
There are many reasons why so many of us have such poor postural alignment. Some problems can be congenital (problems we are born with). Others are the result of compensations that occurred after old injuries or even due to disease. Most commonly though, our poor alignment has been caused by positions we adopt as part of our occupation and/or lifestyle.
Over the years, clinicians have attempted to identify & classify types of problem. Experts such as Janda, Kendall & Sahrmann have identified several postural archetypes which include; Kyphosis/Lordosis, Flat back, Sway back, Military and upper crossed syndrome.
This in my opinion, has been very useful as it has helped information to be passed on to other therapists. In this article, I have only included the examples that I regularly see. I have therefore excluded things such as Military posture. I just never see it and would rather speak from experience.
In addition to putting a name to different problems, experts have been able to identify which structures (muscles, ligaments) are elongated or short in each posture type. I have included some of this information below.
Please bear in mind that not everyone with poor posture fits these models. When it comes to which muscles are elongated and which are shortened, not everyone is the same. At present, I am working with four people with Sway back posture. Two of them have very short hamstrings, the other two can actually do the front splits.
People will often have a combination of problems. For example, people with Sway Back or Lordosis usually have a Kyphosis too.
As alluded to above, muscle length is not the only contributing factor when it comes to body alighnment issues. Connective tissue, joint mobility and anatomical variations such as bone shape and bad habits can also play a part.
I also feel that it’s important not to get to bogged down into the minutia of which muscles are short and which are long. All that really matters is what corrects the problem and what doesn’t. Having said that, I think it often helps to have a reference point which is one of the purposes of this article.
Ideal postural alignment.
Before we plunge into the different types of bad posture, we need to look at what ideal postural alignment looks like. For more details on ideal postural alignment please see here.
[envira-gallery id=”493″]
Common example of poor posture
Lordosis
 The term Lordosis actually refers to the normal curvature of the lower spine (Lumbar spine). When most people talk about a Lordosis they are referring to an increase in this curve (a Hyperlordosis). This is usually caused by the pelvis tilting forwards (anterior tilt) which increases the curve in the spine. The ASIS (anterior suprailiac spine) will be forward of the pubis synthesis and significantly lower than the PSIS (posterior suprailiac spine) (see picture below). People who have a Hyperlordosis usually also have Kyphosis (see section below). This is because everything above and below has to adapt to the position on the pelvis and lower back.
The term Lordosis actually refers to the normal curvature of the lower spine (Lumbar spine). When most people talk about a Lordosis they are referring to an increase in this curve (a Hyperlordosis). This is usually caused by the pelvis tilting forwards (anterior tilt) which increases the curve in the spine. The ASIS (anterior suprailiac spine) will be forward of the pubis synthesis and significantly lower than the PSIS (posterior suprailiac spine) (see picture below). People who have a Hyperlordosis usually also have Kyphosis (see section below). This is because everything above and below has to adapt to the position on the pelvis and lower back.
Possibly shortened muscles: Lower Erector Spinae, Latissimus Dorsi, Quadratus Lumborum, Posterior fibres of the Internal Oblique, Psoas major & Illacus (Hip flexors), Rectus Femoris, Sartorius & TFL (Tensor Facia Latae, the coffee of muscles 😛 ).
Possibly lengthened muscles: Rectus Abdominis, External Oblique, Anterior fibres of Internal Oblique, Gluteus Maximus & Hamstrings.
Sway Back
![]() In Sway Back posture the pelvis is level (not tilted) and displaced anteriorly (shifted forward). Although Sway Back can look a lot like a Hyperlordosis, there is a important difference. A person with a Hyperlordosis will have an increase in the curve of their lower spine (Lumbar spine). Whereas, someone with Sway Back will actually have a flattened Lumbar spine. This is because the pelvis is level (not tilted) and just shifted forwards. There is also usually a degree of Kyphosis.
In Sway Back posture the pelvis is level (not tilted) and displaced anteriorly (shifted forward). Although Sway Back can look a lot like a Hyperlordosis, there is a important difference. A person with a Hyperlordosis will have an increase in the curve of their lower spine (Lumbar spine). Whereas, someone with Sway Back will actually have a flattened Lumbar spine. This is because the pelvis is level (not tilted) and just shifted forwards. There is also usually a degree of Kyphosis.
Possibly shortened muscles: Internal Oblique, Rectus Abdominis & Hamstrings.
Possibly lengthened muscles: Lower Erector Spinae, External Oblique & Gastrocnemius.
Flat Back
![]() Flat back posture is almost like a toned down version of Sway Back. Again the pelvis is level and displaced slightly anteriorly (shifted forward). Unlike Sway back, there is no Kyphosis. I tend to think of Flat back as a Sway Back posture in the making.
Flat back posture is almost like a toned down version of Sway Back. Again the pelvis is level and displaced slightly anteriorly (shifted forward). Unlike Sway back, there is no Kyphosis. I tend to think of Flat back as a Sway Back posture in the making.
Possibly shortened muscles: Rectus Abdominis & Hamstrings.
Possibly lengthened muscles: Lower Erector Spinae.
Kyphosis
 A Kyphosis is an increase in the normal curve of the Thoracic spine. The shoulder blades are often abducted (spread further apart) and the head is held in forward carriage (see ‘Forward Head Posture‘). In rare cases, a Kyphosis can be caused by Scheuermann’s disease, nutritional deficiencies or even be congenital. Most of the time though, it is purely due to slouching or a result of another postural imbalance. As mentioned above, Kyphosis often goes hand in hand with ‘Hyperlordosis‘ and ‘Sway Back‘. A lot of the time, one of these two postures is the cause of the Kyphosis.
A Kyphosis is an increase in the normal curve of the Thoracic spine. The shoulder blades are often abducted (spread further apart) and the head is held in forward carriage (see ‘Forward Head Posture‘). In rare cases, a Kyphosis can be caused by Scheuermann’s disease, nutritional deficiencies or even be congenital. Most of the time though, it is purely due to slouching or a result of another postural imbalance. As mentioned above, Kyphosis often goes hand in hand with ‘Hyperlordosis‘ and ‘Sway Back‘. A lot of the time, one of these two postures is the cause of the Kyphosis.
Possibly shortened muscles: Latissimus Dorsi.
Possibly lengthened muscles: Upper Erector Spinae.
Note: If the shoulder blades are abducted other muscles will be involved.
Scoliosis
 A Scoliosis is defined as an abnormal twisting or sideways curvature of the spine (when viewed from behind). There may also be uneven shoulder or hip heights. There are two main types of Scoliosis, ‘Congenital’ (someone was born with it) or ‘Idiopathic’ (the cause is unknown).
A Scoliosis is defined as an abnormal twisting or sideways curvature of the spine (when viewed from behind). There may also be uneven shoulder or hip heights. There are two main types of Scoliosis, ‘Congenital’ (someone was born with it) or ‘Idiopathic’ (the cause is unknown).
With a congenital Scoliosis, there are often abnormalities around the ribcage such as a hump or concave depression. Occasionally, a hump may be behind a shoulder blade which can cause it to wing (stick out).
I prefer to refer to a Idiopathic Scoliosis as ‘Acquired’. If someone wasn’t born with the condition then they must have acquired it somehow. Often, the spine has just adapted to a behaviour. If someone sits on one hip with their legs out to the side for long enough, their spine will adapt to the position.
The same can be said for people who are unlucky enough to have jobs where they constantly have to lean or twist in one direction (Think production lines workers, checkout staff, carpet fitters). Even carrying a baby on one hip, if done for long enough, will affect the alignment of your hips and spine.
In a lot of cases, an acquired Scoliosis has developed due to another part of the body being out of alignment. A flattened arch of a foot effectively shortens one leg, this tips the pelvis over on one side which has a knock on affect up the spine.
I also regard a ‘true’ leg length discrepancy (a difference in bone lengths) as acquired. Admittedly.. the leg length discrepancy was congenital. When the person was born though, their spine was straight. It wasn’t until they started walking around that they acquired the Scoliosis.
When it comes to which muscles are lengthened or shortened, each case is unique. Pretty much any muscle around the body can be effected. There will be shortened muscles on the inside of a curve and lengthened muscles on the outside of a curve. The same applies to a rotation, one oblique muscle may be lengthen and the opposite one shortened.
Rather than fixating on which muscles are long or short I think it’s initially more important to work out the true cause of the problem.
Pelvic Malalignment
 A Pelvic Malalignment manifests itself in several different ways. To my knowledge, there is no widely used term for this collection of problems. I have therefore, chosen to use the term Pelvic Malalignment in this article. I have also limited this article to the types of malalignment I most commonly see. Namely, a pelvic height imbalance with or without rotation.
A Pelvic Malalignment manifests itself in several different ways. To my knowledge, there is no widely used term for this collection of problems. I have therefore, chosen to use the term Pelvic Malalignment in this article. I have also limited this article to the types of malalignment I most commonly see. Namely, a pelvic height imbalance with or without rotation.
In addition to problems around the pelvis, a Pelvic Malalignment can also have a knock on effect on other part of the body. In some cases, the Pelvic Malalignment may actually have been caused by a problem in one of these areas. It is also not uncommon for someone with this type of problem to also have some degree of ‘Scoliosis‘.
Like a ‘Scoliosis‘ (see above), the underlying cause of the pelvic malalignment is often complex and specific to an individual. Rather than just provide a list of affected muscles, I have chosen to briefly outline the characteristics of this flavour of poor posture.
Signs of Pelvic Malalignment.
There will be a difference in pelvic height on one side (One ASIS will be lower than the other ASIS). In addition:
The pelvis may have tilted forwards on one side. If this is the case, the ASIS will be significantly lower than the PSIS on the effected side.
The entire pelvis may have rotated horizontally (the transverse plane). Simply put, one side of the pelvis will be further forward than the other.
Often, these problems all occur together. I do however, occasionally see people with just one of the above signs. I will probably delve in to each one individually and explore other types of Pelvic Malalignment in coming articles.
Forward Head Posture AKA ‘Text neck’
 This is probably the most common problem I see. The head is held in forward carriage (out in front of the body). This increases the Lordosis (curvature) of the neck. Forward head posture is often seen alongside ‘Kyphosis‘, ‘Upper crossed Syndrome‘ and ‘Medially Rotated Arms‘ (see sections). It can also be a sign of Osteoporosis.
This is probably the most common problem I see. The head is held in forward carriage (out in front of the body). This increases the Lordosis (curvature) of the neck. Forward head posture is often seen alongside ‘Kyphosis‘, ‘Upper crossed Syndrome‘ and ‘Medially Rotated Arms‘ (see sections). It can also be a sign of Osteoporosis.
Possibly shortened muscles: Any/all of the muscles that extend the upper neck, flex the lower neck and protract the head: Levator Scapula, Upper Trapezius, Sternocleidomastoid, Splenius Capitis, Semispinalis Capitis, Longissimus Capitis, the Anterior/Medial Scalenes and the Suboccipital muscles.
Possibly lengthened muscles: Any/all of the muscles that flex the upper neck, extend the lower neck and retract the head: Semispinalis Cervicis, Splenius Cervicis, Longissimus Cervicis, Rectus Capitis Anterior, Longus Capitis, Suprahyoid muscles.
Upper Crossed Syndrome
20-23") A Therapist called Dr Vladimir Janda first coined the phrase Upper Crossed Syndrome back in the 80’s. Hopefully the picture explains where the name came from. The shoulders are rounded forwards and often, the head is held forwards of the body (see ‘Forward Head Posture‘ above).
A Therapist called Dr Vladimir Janda first coined the phrase Upper Crossed Syndrome back in the 80’s. Hopefully the picture explains where the name came from. The shoulders are rounded forwards and often, the head is held forwards of the body (see ‘Forward Head Posture‘ above).
Dr Janda classified the following muscles as shortened (& facilitated) or lengthened (& inhibited). ‘Facilitated’ can be defined as over active whereas, ‘Inhibited’ means the muscle is under active.
The following is Janda’s list.
Shortened & facilitated muscles: Chest muscles (Pectoralis Major & Minor), Sternocleidomastoid, Upper Trapezius & Levator Scapula.
Lengthened & inhibited muscles: Deep cervical (neck) flexors, Lower Trapezius & Serratus Anterior.
As mentioned in the introduction to this article, in my experience not everyone with bad alignment fits these models. In this case, I actually find that the upper Trapezius is often inhibited. In fact, if the shoulder blades are abducted (more than 3″ from the spine), then the whole of the Trapezius could be lengthened and inhibited. The Rhomboids may also be lengthened.
With the shoulders rounded and forwards, the Trapezius & Rhomboids cannot function properly. This leads to other muscles taking over during a lot of everyday movements.
People with Upper Crossed Syndrome often have ‘Medially Rotated Arms‘ too (see below).
Medially Rotated Arms
 Simply put, the arms are rotated inwards with the back of the hands facing forwards. The thumbs should be facing straight ahead. Medially rotated arms usually go hand in hand (excuse the obvious pun) with Upper Cross Syndrome (see above). If this is case, some of the same muscles will be shortened or lengthened.
Simply put, the arms are rotated inwards with the back of the hands facing forwards. The thumbs should be facing straight ahead. Medially rotated arms usually go hand in hand (excuse the obvious pun) with Upper Cross Syndrome (see above). If this is case, some of the same muscles will be shortened or lengthened.
People’s weight can play a factor. If a person is very overweight, the angle their arms hang at their sides will be effected. If this person tried to put their shoulder in the correct position their body would get in the way. To get around this problem the shoulder blades spread apart (abduct) which causes the arms to appear medially rotated.
Possibly shortened muscles: Pectoralis Major, Latissimus Dorsi, Teres Major & Subscapularis.
Possibly lengthened muscles: Teres Minor & Infraspinatus.
There are occasions when the arms are still medially rotated even when the shoulder position has been corrected. If this is case then the muscles of the forearm or even upper arm will most likely be the culprits.
Downwards Rotated Shoulder Blades
 Downwardly rotated means that the inferior (lower) angle of the shoulder blade is closer to the spine than the upper medial border (see the red dots in the picture).
Downwardly rotated means that the inferior (lower) angle of the shoulder blade is closer to the spine than the upper medial border (see the red dots in the picture).
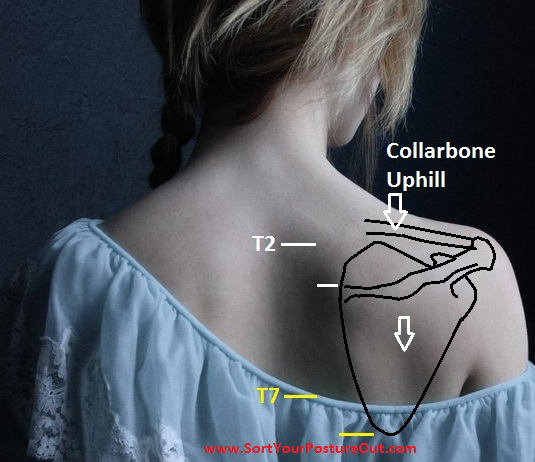
The whole shoulder is usually slightly dropped and sitting lower on the ribs than it should be. The collar bone will be running uphill or flat, instead of running downhill from arm to chest (the same as a depressed shoulder/ see pic below).
The next bit is a bit complicated…If a shoulder blade is downwardly rotated, the arm won’t be hanging in its normal position. The side of the body will have blocked the arm from maintaining proper alignment. This means that there will be an increased angle between the shoulder blade and the arm. When the shoulder blade position is corrected, the persons arm is often left hanging out away from their side (abducted). This is because the muscles of the shoulder have adapted to the position the shoulder blade is in and have shortened.
This a lot more common than most people think and something I see very regularly. A person with a downwardly rotated shoulder blade often has shoulder pain or may have nerves issues in their hand or arm (Thoracic outlet syndrome).
Possibly shortened muscles: Chest muscles (Pectoralis Major & Minor), Levator Scapula, Rhomboid, Deltoid, Supraspinatus, Latissimus Dorsi & occasionally Lower Trapezius.
Possibly lengthened muscles: Upper Trapezius, Serratus Anterior & occasionally Infraspinatus/Teres minor.
Depressed Shoulders
 A depressed shoulder is not a happy shoulder. The shoulder blade is sitting lower than it should be. A person with this problem may appear to have a long neck.
A depressed shoulder is not a happy shoulder. The shoulder blade is sitting lower than it should be. A person with this problem may appear to have a long neck.
In their normal position, the top of the medial border should be level with T2 (the 2nd Thoracic vertebra down). The bottom of the shoulder blades should be the same height as T7 (the 7th Thoracic vertebra down). Basically the two white lines and two yellow lines in the picture should line up.
The collar bone will also be running uphill or flat, instead of running downhill from arm to chest (which is the norm). A shoulder can be classified as depressed if:
The rotationally alignment of the shoulder blade is normal (see Downwardly Rotated Shoulder Blades) and the shoulder is below T2-T7.
Possibly shortened muscles: Chest muscles (Pectoralis Major & Minor) & Latissimus Dorsi.
Possibly lengthened muscles: Upper Trapezius & Serratus Anterior.
Elevated Shoulders
 This is the opposite of a ‘Depressed Shoulder‘, still not a happy shoulder though! Someone with this type of posture will be locked in a permanent shrug. Typically, I find that it’s just one shoulder that is raised (often the keyboard hand). This is another complicated one so here is a quick recap of normal shoulder positioning.
This is the opposite of a ‘Depressed Shoulder‘, still not a happy shoulder though! Someone with this type of posture will be locked in a permanent shrug. Typically, I find that it’s just one shoulder that is raised (often the keyboard hand). This is another complicated one so here is a quick recap of normal shoulder positioning.
As mentioned here the normal positioning of the shoulder girdle is as follows:
The medial border of the scapula spine should be around 3″ from the Thoracic spine and closer to spine than the bottom of the shoulder blade.
The shoulder blades height should be between T2 (the 2nd Thoracic vertebra down) & T7 (the 7th Thoracic vertebra down).
The collar bone should run slightly downhill from arm to chest.
If a shoulder blade is elevated, the top of the medial border will be above T2 & the bottom will be higher than T7. The collar bone will also be running more steeply that it should be. Still with me? Here is where it get complicated. The rotation of the shoulder blade and distance from the spine dictates which muscles are short or long.
If the medial border of the scapula spine is elevated, then the Levator Scapula will be short. Note: The shoulder blade may appear to be Downwardly Rotated (see above). The difference is that in this case the top of the medial border is above T2.
If the entire shoulder blade is elevated then the upper Trapezius will be shortened. If this is the case the collar bone will be running steeper than it should from arm to chest.
If the entire shoulder blade is elevated and closer to the spine than 3″ then the Levator Scapula, upper Trapezius and Rhomboid will all be short.
Winged Shoulder Blades
 Winging means that the shoulder blades are not sat flat against the rib cage. The inside border of the shoulder blades will be noticeably sticking out. I have actually been able to fit my fist between the shoulder blade and ribs of some people (Always a head turner that one 😛 ).
Winging means that the shoulder blades are not sat flat against the rib cage. The inside border of the shoulder blades will be noticeably sticking out. I have actually been able to fit my fist between the shoulder blade and ribs of some people (Always a head turner that one 😛 ).
Note: Winging refers to the whole inside border sticking out, not just the bottom corner. If it is just the bottom corner, then a short pec minor is the chief culprit.
In rare cases a winged scapula may have be caused by damage to the long thoracic nerve. Most of the time though, is just down to bad habits and incorrect passive muscle length or stiffness.
Possibly shortened muscles: Chest muscles (Pectoralis Major & Minor), Bicep & Latissimus Dorsi.
Possibly lengthened muscles: Mid/lower Trapezius & Serratus Anterior.
Depending on the rotation of the arms, the muscle length of the deltoid and rotator cuff may also be involved.
Duck Feet
 Someone with Duck Feet has feet that are externally rotated (turned out) and not facing straight ahead. A turned out foot causes the arch of the foot to flatten. This in turn, reduces the amount of shock absorption we have when we run.
Someone with Duck Feet has feet that are externally rotated (turned out) and not facing straight ahead. A turned out foot causes the arch of the foot to flatten. This in turn, reduces the amount of shock absorption we have when we run.
Having a flattened arch also effectively shortens the length of the leg. This can have a knock on effect up the entire body (see Scoliosis). People with turned out feet are also more likely to suffer knee, hip and back injuries (especially if they are runners).
As for what is physically going on, the problem can originate at the hip, knee or ankle.
If the problem starts at the hip, the whole leg will be externally rotated (the knees will point slightly outwards). Typically the deep external rotators of the hip such as Piriformis will be short. The larger bum muscles such as Gluteus Maximus will often be under recruited.
Although the knee is usually classified as a hinge joint, it does have a degree of rotation. On occasions, the Bicep Femoris (one of the hamstring muscles on the back of the upper leg) can be become shortened. This causes the tibia to rotate outwards.
The problem can also be caused by a lack of range of motion in the ankle. If the joints in the foot/ankle don’t have enough movement, a person will turn their foot out so they can walk. This can also be caused by tight muscles. If the calf muscles (Gastrocnemius & Soleus) are short, the range of motion in the ankle will be reduced. The body often follows the path of least resistance and keeps us moving.
Most of the time this problem is caused by habit and is more common in men. There are however, bone abnormalities that cause this problem. If someone has a retroverted hip (the neck of the femur is twisted out of normal alignment) then they will turn their foot outward to put their hip joint in a better position. There is also a condition known as External Tibial Torsion (a twisting of the shin bone) that can also cause someone to have a duck foot.
You can read more about duck feet in the article ‘Why your turned out duck feet are trashing your body’.
In closing
As I mentioned under the heading ‘Bad Posture’, not everyone fits the models above. For this reason, I have used terms such as ‘Possibly shortened/lengthened’ throughout this article. Please don’t presume a muscle is short or long just because it is listed above as so.
Poor body alignment has many causes and cases are often unique. If you are worried about your posture, I recommend going to see a muscularskeletal specialist (such as a Physical Therapist) to get yourself checked out. At the very least they should be able to assess your body alignment and tell you what is truly short, long, or not working at it’s best.
Some of the images included in this article are from ‘Muscle Testing and function with Posture & Pain’ by Kendall, Provance, Rogers & Romani. If this floats your boat you can get hold of a copy here.
How can kyphosis be corrected
This is an excellent explanation of alignment issues in the body. I have had a bad back and hips for as long as I remember. I have always been told that I walk funny and stomp when I walk. I have had a sore back and hips for a long while too. It was pointed out that my feet point outwards quite a bit and that I have an extreme curve in my lower back. When I lay down flat I can roll a golf ball under my lower back. After my back going out again the other week, I decided to make the next step and book to see a Phisical Therapist. My first appointment is in two weeks. I will tell them everything I can and hope they can start getting me onto the road to correcting this (I’m thinking a long one). Hopefully they can help me correct my posture and get me walking like a normal person. This article has shown me a lot of what can go wrong to throw you body out of order. Thank You.
This is fantastic Dr Lloyd. The viuasl guide puts things into perspective for the general population and ultimately gives them ways to improve the posture. I also liked the reasons for bad posture and how not all are physical. I think more emphasis should be placed on the connection between mental state and bad posture as this is engrained into a person, however I am not a medical professional so am not able to provide diagnosis or anything like that. This was great information, thank you so much. I will be referencing it in my blog post, I hope that’s ok.
Thanks for your comments. My name is not Dr Lloyd though.